

Wrist and thumb pain: Possible signs of de Quervain’s Tenosynovitis
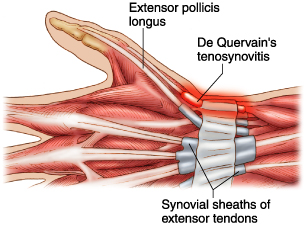
There are many causes of wrist pain. One cause is a condition called de Quervain’s tenosynovitis, which is inflammation of the synovial tendon sheaths (protective sleeves) of two tendons, extensor pollicis brevis (EPB) and abductor pollicis longus (APL) as they pass over the wrist (Fig 1). These two tendons are responsible for moving the thumb therefore it commonly occurs in people who perform repetitive movements of the wrist and thumb.
Fig 1. Anatomy of the wrist
Some well known causes include:
· Repetitive physical work with the hands
· Excessive writing
· Excessive typing
· Racquet sports
· Rowing
Interestingly it also occurs in mothers with newborns and toddlers. Repetitively lifting a child from under the armpits results in excessive load on the EPB and APL tendons. Such strain can also occur whilst performing hammer curl exercises with dumbbells.
Behaviour modification and reducing aggravating factors are usually the best way to settle de Quervain’s tenosynovitis. Wearing a wrist brace can be suggested, but this is not an ideal long-term solution.
Pacing, although a principle used for chronic pain conditions, can be applied as it teaches you to limit and control your aggravating activities. See video below.
Ice and non-steriodal anti-inflammatories (NSAIDS) can be trialed but if the aggravating activities are not addressed, this is unlikely to result in lasting relief.
All of these factors can be identified in a detailed physiotherapy assessment. Some milder cases of de Quervain’s tenosynovitis are responsive to specific exercises, massage and/or dry needling to the forearm and wrist muscles.
De Quervain’s tenosynovitis can be responsive to an ultrasound guided cortisone injection. Surgical release of the tendons can be offered in rare cases.
If you think you have de Quervain’s tenosynovitis, see a doctor or physiotherapist for a detailed assessment and treatment recommendations.

Daniel Di Mauro graduated with a Bachelor of Physiotherapy from La Trobe
University in 2008. He commenced his career immediately in private practice
with an interest in workplace injuries and multidisciplinary pain management.
Daniel completed a post-graduate credentialing in the McKenzie Method of
Mechanical Diagnosis and Therapy in 2011 and is a current member of
McKenzie Institute Australia.
He still remains active in clinical research as a treating physiotherapist in the
La Trobe University Multidirectional Shoulder Instability trial which is
comparing the Lyn Watson and Rockwood rehabilitation programs for people
with atraumatic multidirectional shoulder instability.
Daniel’s experience has given him strengths in the areas of chronic pain, low
back pain, shoulder pain, worksite assessments and functional capacity
assessments.
Daniel is able to speak Italian.